|
Abstract
Background:Among concerned nasal appearances, a deformity
with supero-lateral displacement of the nostril rim,
called retracted nostril rim or elevated nostril rim,
is commonly seen and considered one of the most difficult
ones to treat aesthetically.
Methods: A new surgical method for treating retracted
nostril rim was performed in 10 patients, utilizing
the combination of auricular composite graft, internal
fixation with a retainer, and external continuing
suspension with anchoring sutures.
Results: The procedure was successful in maintaining
the grafted cartilage in the ideal position and avoiding
recurrence of retraction or elevation of the constructed
alar rim.
Conclusions: The presented method merits consideration
as a standard operative approach for correction of
retracted nostril rim.
Keywords:
elevated nostril rim, retracted ala, cartilage graft,
external suspension, retainer
Introduction
The shape of the nostril rim is a very sensitive topic,
especially among women. Retracted or elevated (supero-lateral
displacement) nostril rim occurs congenitally, or
iatorgenically due to scar contracture after various
kinds of rhinoplasty. Gunter et al. [1] previously
suggested a definition of retracted ala as a deformity
characterized by an alar rim to nostril long axis
distance of more than 2 mm. Retracted alar rims make
the nostrils appear too big, and nasal hair be seen
from oblique and lateral views. As for the unilateral
cases, the most common complaint is a marked difference
in the size and shape of the nostril rim. Morphologically,
retracted nostril rims can be classified into two
types: Type I includes those cases where the nostril
rim is completely displaced supero-laterally and the
nasal cavity can be seen from the frontal view. Type
II includes those cases where part of the nostril
rim is supero-laterally displaced and appears to be
notched. Type I occurs congenitally and is usually
bilateral, while type II occurs both congenitally
and iatrogenically, and iatrogenical cases involve
usually only one side.
Although retracted nostril rims are seen frequently
and there have been several surgical techniques and
their modifications for it, it is still considered
as one of the most difficult nasal deformities to
treat. Meyer and Kesselring [2] introduced a method
for lowering the alar rim with a graft of alar cartilage
strip, and Ellenbogen [3] modified it as a combined
technique with a local skin flap and a cartilage graft
(septal, lower lateral, or auricular). But this method
left a raw surface on the internal mucosa, which could
lead to postoperative complications like distortion,
retraction, and protrusion of the grafted cartilage.
Guyuron [4] used an internal V-to-Y advancement with
or without a cartilage graft for the severe alar retraction,
and Rohrich et al. [5] utilized alar contour grafting
with septal cartilage. Constantian [6] used Sheen
and Sheen's method [7] with minor modifications and
showed relatively successful results by using skin
and cartilage composite grafts harvested mainly from
the auricle for secondary or tertiary rhinoplasty.
Based on our experiences, insufficient improvements
or postoperative retractions can be seen especially
in severe cases of retracted alar rim deformity or
in the cases with scaring.
The authors modified the methods above to try to avoid
postoperative retraction of the nostril rim by combining
auricular composite grafts and postoperative anchoring
suspension.
Subjects
A total of 10 patients, including 9 females and 1
male, were treated with the present method. The age
of the patients ranged from 21 to 44 (mean ü} SD: 32.2
ü} 7.0). All 6 bilateral cases did not have any history
of rhinoplasty, while 4 unilateral cases are composed
of 2 congenital cases and 2 iatrogenic ones. Eight
congenital cases are composed of 5 Type I cases and
3 Type II cases, while two iatrogenic cases showed
Type II deformity. The follow-up periods ranged from
5 to 20 months. The summarized data are shown in Table
1.
Surgical Technique
First, an auricular cartilage and its adherent anterior
skin is harvested from the posterior conchal wall
as a composite graft (Fig. 1A). For bilateral cases,
the combined skin and cartilage grafts are harvested
from the anterior surface of both auricles while for
the unilateral cases it is harvested from a single
side. The skin defect is closed with 7-0-nylon, while
the cartilage defect is left as it is.
The combined skin and cartilage graft is trimmed and
fabricated to match the preoperative design of the
recipient site. The cartilage is shaved to about one-half
original thickness to avoid postoperative bulky appearance
of nasal ala. After completion of the fabrication,
two 7-0-nylon sutures for anchoring suspension are
passed through the end of the cartilage on the side
placed to the alar margin (Fig. 1A).
A little cephalic from the hair-bearing margin of
the vestibular skin, a rim incision is made followed
by undermining in the caudal direction to form a skin
pocket and unfurl the alar margin caudally (Fig. 1B,
1C). The free ends of the two 7-0-nylon anchoring
sutures are passed out through the nostril rim skin
for proper positioning and postoperative suspension
of the auricular composite graft. Once positioned
in the skin pocket, the composite graft is fixed with
sutures followed by skin closure (Fig. 1E). In order
to stabilize the graft, a nasal retainer is inserted
into the nasal cavity followed by an external fixation
with a plastic cast (AquaplastR A962-54, Smith &
Nephew Inc., WI). The final procedure is to fix the
free ends of the 7-0 nylon sutures to the cast with
tape (MicroporeR, 3M, MN) to avoid cephalic displacement
of the graft (Fig. 1D, 1F). The internal retainer
and the external cast as well as the anchoring sutures
are removed 1 week after surgery.
Cases
Case 1: A 36-year old female patient with bilateral
retracted nostril rim classified as Type I. The patient's
chief complaint was that the nasal cavity can be seen
from the front (Fig. 2A). A combined skin and free
composite cartilage graft was harvested from the anterior
surface of both auricles with the dimension of 18
x 4 mm. The graft stabilized without any post-operative
complications or problems. At 7 months, a natural
configuration of the nostril rim was attained with
symmetry and the patient was satisfied with the result.
The nasal cavity was relatively concealed from the
frontal view (Fig. 2B).
Case 2: A 21-year old female patient
with bilateral retracted nostril rim classified as
Type II. The pre-operative frontal appearance revealed
a notch-like configuration in the superior region
of the nostril rim (Fig. 3A). The post-operative appearance
at 5 months revealed that the notch-like configuration
had been sufficiently corrected and that a natural-looking
configuration of the nostril rim had been attained
(Fig. 3B).
Case 3: A 28-year old female patient
with right unilateral retracted nostril rim classified
as Type II. The pre-operative frontal view showed
asymmetry of the nostril rim, especially the notch-like
configuration located in the superior region of the
right nostril rim (Fig. 4A). A combined skin and free
composite cartilage graft was harvested from the anterior
surface of the right auricle. The right nostril rim
was successfully corrected without any postoperative
complications, and a natural-looking configuration
of the right nostril rim and symmetry had been maintained
at 15 months (Fig. 4B).
Results
In all 10 cases, improvement of the retraction and
patient satisfaction were obtained with minimal variation.
Postoperative recurrence of the deformity was not
clearly detected during the follow-up periods ranged
from 5 to 20 months. Bulkiness of the ala was seen
in one case in which the auricular cartilage was not
thinned. In two cases localized focal necrosis of
the skin cover of the cartilage graft was seen at
1 week after surgery, and yet left no postoperative
alar deformity.
Discussion
The nasal ala has a freed margin, and this is one
of the reasons for difficulty in correcting alar deformity,
suggesting the importance of postoperative fixation
of the reconstructed ala during the healing period.
The authors combined the auricular composite graft
to the internal fixation with a nasal retainer and
the external continuing suspension with anchoring
sutures. For cast fixation, we used cast plastic with
heat, but other materials such as Denver SplintR (Shippert
Medical Technologies, CO) can be used. Continuing
suspension of the grafted cartilage greatly helps
it maintained in the ideal position of the nasal ala.
It also should be noted that the skin pocket of the
recipient site is undermined in the caudal direction
to construct a deep pocket, to obtain a tensility
of the skin cover, and to allow for easy unfurling
of the vestibular skin.
In our procedure, the composite graft was harvested
from the anterior aspect of the auricle. This is due
to the fact that the volume of the skin cover and
subcutaneous soft tissue of the posterior surface
is thicker in comparison to that of the anterior.
If the composite graft taken from the posterior surface
is utilized for the nostril rim, a bulky appearance
is unavoidable. For the same purpose, the harvested
cartilage is to be shaved to about one-half original
thickness. If the harvested cartilage is used in its
original form, the cartilage is thick and hard, and
can be visible or felt at the external skin surface.
In addition, when harvesting the composite graft,
it is important to select an area of the auricle that
closely resembles the curved configuration of the
nostril rim and thus we use the posterior wall of
the concha.
Some of congenital bilateral type I cases are partly
due to the short nose as suggested by Case 1. Although
the present method does not improve the short nose,
it can correct the large-looking appearance of the
nostril frequently accompanying it.
Though further accumulation of cases is necessary,
we believe that the presented method merits consideration
as a standard operative approach for correction of
retracted nostril rim.
Legend:
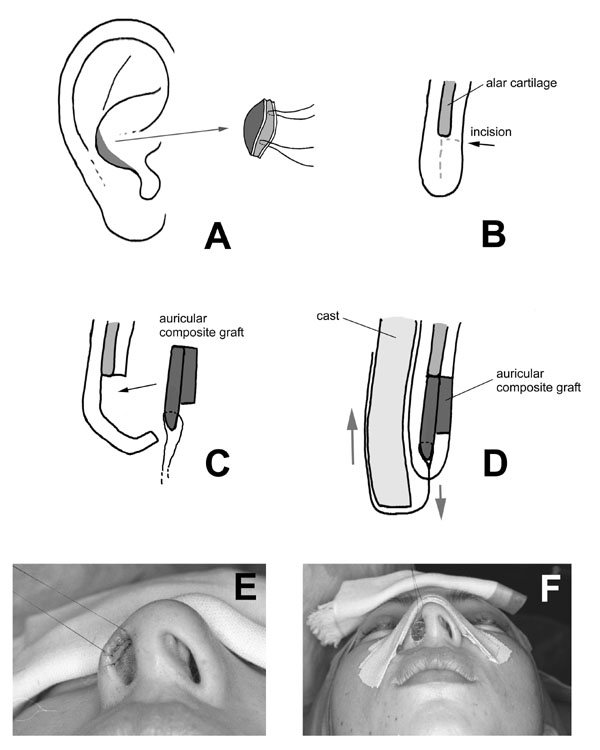
Fig. 1. Surgical procedure.
A:The donor site of the auricular composite graft.
Two 7-0 nylon sutures for anchoring suspension were
passed through the lateral end of the cartilage.
B-D: Cross-sectional views of the nasal ala.
E: The composite graft was sutured to the recipient
site and the anchoring sutures were passed out through
the nostril rim skin.
F: The reconstructed ala was fixed with an internal
retainer and an external cast on which the anchoring
sutures were fixed with taping.
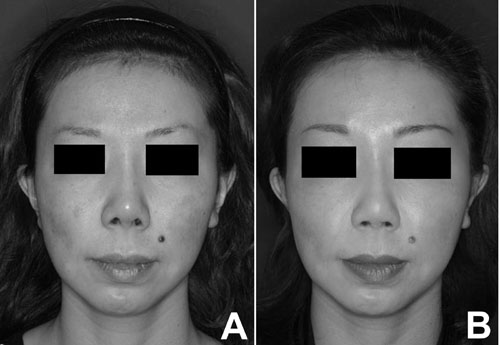
Fig. 2. Case 1. A 36-year old female patient with
bilateral retracted nostril rim classified as type
I. A: a preoperative frontal view., B: a postoperative
frontal view at 7 months.

Fig. 3. Case 2. A 21-year old female patient with
bilateral retracted nostril rim classified as type
II. A: a preoperative frontal view., B: a postoperative
frontal view at 5 months.

Fig. 4. Case 3. A 28-year old female patient with
unilateral retracted nostril rim classified as type
II. A: a preoperative frontal view., B: a postoperative
frontal view at 15 months.
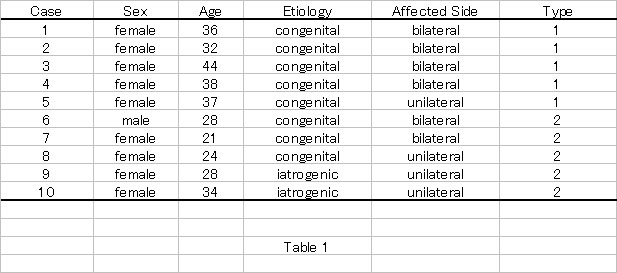
Table 1. Summarized data of cases
References
1. Gunter JP, Rohrich RJ, Friedman RM: Classification
and correction of alar-columellar discrepancies in
rhinoplasty. Plast. Reconstr. Surg. 97: 643-648, 1996.
2. Meyer R, Kesselring UK: Sculpturing and reconstructive
procedures in aesthetic and functional rhinoplasty.
Clin. Plast. Surg. 4:15-39, 1977.
3. Ellenbogen R: Alar rim lowering. Plast. Reconstr.
Surg. 79: 50-57, 1987.
4. Guyuron B: Alar rim deformities. Plast. Reconstr.
Surg. 107: 856-863, 2001.
5. Rohrich RJ, Raniere J, Ha RY: The alar contour
graft: correction and prevention of alar rim deformities
in rhinoplasty. Plast. Reconstr. Surg. 109: 2495-2505,
2002.
6. Constantian MB: Indications and use of composite
grafts in 100 consecutive secondary and tertiary rhinoplasty
patients: introduction of the axial orientation. Plast.
Reconstr. Surg. 110: 1116-33, 2002.
7. Sheen JH, Sheen AP: Aesthetic Rhinoplasty, 2nd
Ed. St. Louis: Mosby, 1987, Pp. 372-382.
|